

For-Profit Hospice--When Money Becomes the Mission
For-Profit Hospice--When Money Becomes the Mission
The recent Pro-Publica/New Yorker article by Ava Kofman

Several years ago my husband and three children and I were driving through rural Pennsylvania on a family trip and saw a billboard that asked, somewhat ominously: “Is Your Hospice Letting You Down?” It struck me as crass and opportunistic, but also revealing of how commercialized many hospices had become. Ava Kofman’s recent exposé for Pro-Publica/The New Yorker, titled “Endgame: How the Visionary Hospice Movement Became a For-Profit Hustle” explores the contours of that commercialization and the large-scale fraud that has resulted. The article was painful reading for me since I worked as a hospice nurse, for a not-for-profit and a for-profit company. As readers of my book Healing already know, working for a for-profit hospice significantly contributed to my feeling of clinical burnout and moral distress.
Some history of the hospice movement will be helpful before diving into Kofman’s article. First, note the word “movement” in the previous sentence. Profiteering by for-profit hospices resulted from hospice’s transition into a Medicare-funded business, away from a true movement that arose in large part from work done by Dame Cicely Saunders and Dr. Elisabeth Kubler-Ross. The first hospice in America was founded in 1974 in Branford, Connecticut and is still open today, still not-for profit. In 1978 a U.S. Department of Health, Education, and Welfare task force validated hospice as a needed option for dying patients and said that it deserved federal funding. At that time, hospices were mission-driven and staffed by at least some volunteers.
In 1979 The Health Care Financing Administration (HCFA) studied 26 hospices to formalize what hospice care should consist of and to evaluate hospices’ cost-effectiveness. Ronald Reagan signed the Medicare Hospice Benefit into law in 1983, and in 1993 hospice was included in the Clinton health care reform plan, establishing it as part of established health care in the U.S.
Thus, in a few decades, hospice grew from a grassroots, volunteer-dependent approach to end-of-life care to a mandated benefit with essentially guaranteed funding from Medicare. The decision to federally fund hospice care, while supported by the best of intentions, inadvertently offered an open door to entrepreneurs who grew to see hospice as a means to maximize profits from that secure Medicare funding stream.
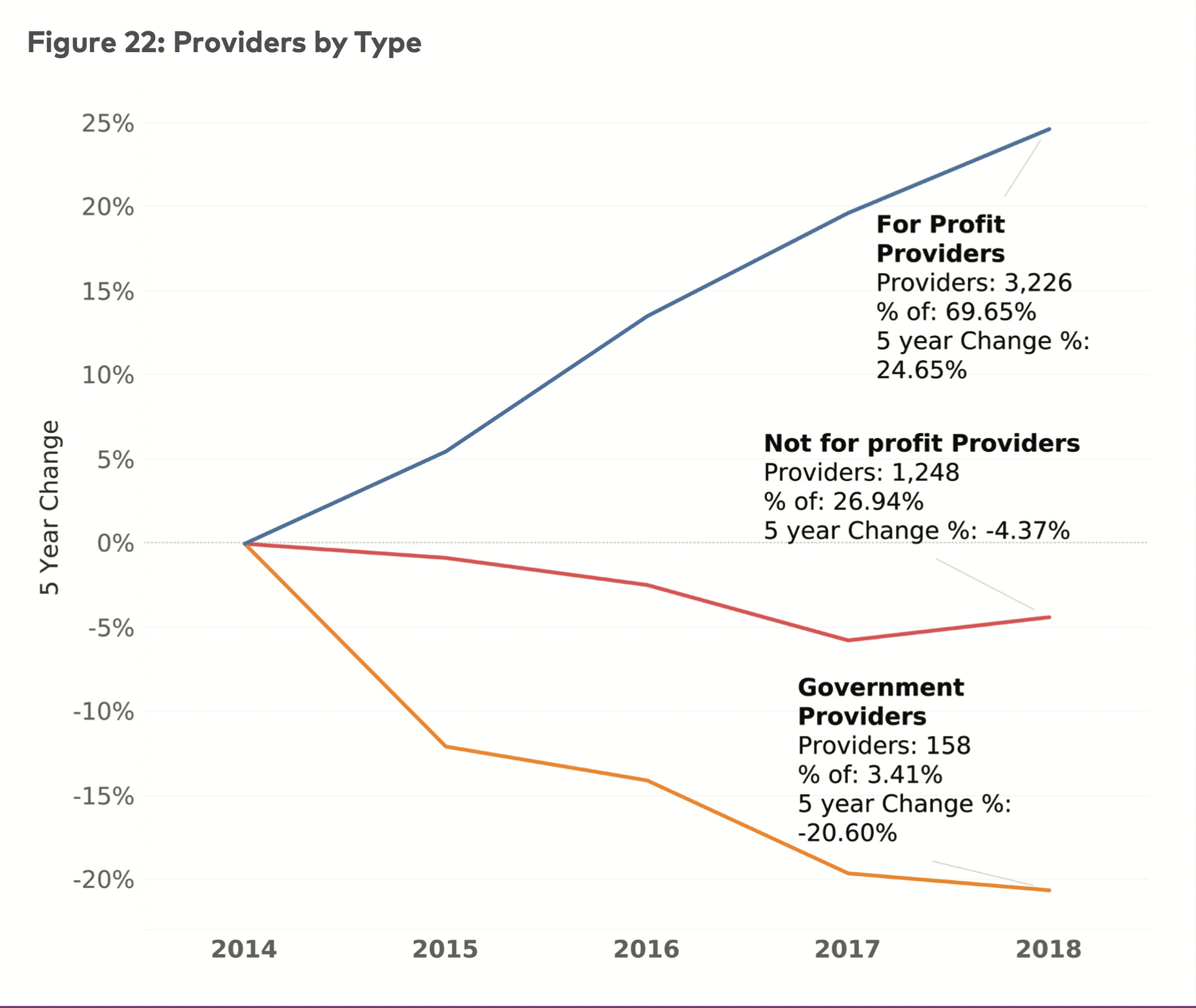
Indeed, the growth of for-profit hospices has been unrelenting over the past few years, as the graph below, from the National Hospice and Palliative Care Association (NHPCO) 2020 report, shows. In 2018, 69.7% of hospice providers had for-profit tax status while just 26.9% had not-for-profit status, an increase of 24.7 % in for-profit hospices since 2014.
Kofman’s article further clarifies that some of the worst hospice actors are owned by Private Equity companies that have no interest in health care beyond money-making. The for-profit hospice I worked for became much more penny-pinching and exploitative of staff after it was bought by a holding company with a diverse portfolio, which is to say, commitment to and concern for patients were subordinated to cost-cutting and profit-making.
The federal hospice benefit created a public-private dyad ripe for exploitation in a way typical of American health care. In the article Kofman quotes James Barger, a lawyer for two hospice whistleblowers, describing the lack of real controls on hospice spending as “a ludicrous amount of optimism in a system with a capitalist payee and a socialist payer.” So much of health care in America has this same problem: combining capitalist health care delivery systems, whether clinics, hospitals, the pharmaceutical industry, or insurance companies, with guaranteed federal money to support those systems. Too many people have learned how easy and profitable it is to game the system, and so they do, but systemically throughout health care in the U.S., not just in hospice.
Kofman’s article is well-researched and important, but it’s also open to critique because it didn’t give any counterexamples, running the risk of turning patients in need away from effective, compassionate hospice care. A good friend who is a hospice executive and a nurse shared her dismay with the article, saying she worried it would make patients and family members already struggling with a life-ending diagnosis resist hospice, denying themselves helpful and needed end-of-life care (thank you, Sarah!). Katie Smith Sloan, President and CEO of Leading Edge, the association of nonprofit providers of aging services, including hospice, published a quite good response to Kofman’s article where she acknowledges the proliferation of for-profit hospices and accompanying fraud. You can read the entire letter here, but below I quote her excellent summary of the real problem—lack of quality care for all of the frail elderly:
“Good hospice care, because of its holistic, patient- and family-centered compassionate approach to the dying, is a godsend. Bad care and true fraud in this valuable benefit are intolerable. Change is needed. Reform must promote high quality care, including the right services in the right quantity, and eliminate opportunity for misdeeds. Most importantly, our country is in desperate need of a system of long-term services and supports that is responsive to how older adults live and die now.”
Aye, there’s the rub: here in the U.S., we do not support elderly patients with chronic illnesses who need constant care, which also means we do not support their families. Instead, we rely on billions of dollars of free care primarily provided by female relatives. We have created a system of elder care ripe for gaming by the greedy and unscrupulous that leaves many struggling patients without the health care they need—a true moral failure.
In the meantime, though, good hospices exist. For anyone in need of hospice care, begin your search for a hospice by looking for a not-for-profit company. That is not a guarantee of quality, but it’s a good stand-in for commitment to the hospice mission. Also remember that you can switch hospices at anytime—settling for care that is deficient is not required. If you can’t find a quality hospice in your area, see if you can work with your primary care provider or a palliative care physician or nurse practitioner to prescribe the medications your dying loved-one needs. That advice will be hard for anyone without health insurance to follow, but Americans over 65 can get Medicare and I suggest pushing for the care needed to help patients die comfortably, and at home if that is their preference.
If readers have ideas to add to my suggestions, please leave a comment. You can also forward this column to colleagues in hospice and see what ideas they may have to help dying patients secure the care they need. I hate to own up to the jury-rigging that can be required to get appropriate end-of-life care, but since that’s true, I encourage people to share what did or did not work for them, or what they have seen work in their own clinical practice. The cartoon below from Rob Chast is ironic, but also a good reminder of what actually matters at the end of life. Well, what she says, plus maybe oxygen, some morphine and Ativan, a hospital bed that works, and a hospice nurse who really cares—they do exist.
Hugs to all as we head in to the holiday season—
Theresa

Congratulations on your last treatment! Hooray! And I agree with the other commenters. That is a beautiful photo of you!
Thankfully, our family hasn’t had to deal with the hospice system yet, but if/when we need it, I am grateful for your suggestions.
Theresa, thank you. Your writings illuminate us to the sad truths about this profession. Hopefully growing public awareness will precipitate the systemic changes needed.